
Basal Cell Carcinoma
WHAT IS BASAL CELL CARCINOMA?
Basal cell carcinoma (BCC) is a slow-growing form of skin cancer, caused by the abnormal growth of basal cells within the skin.
EPIDEMIOLOGY
BCC is the most common cancer in the United States, and the most common type of skin cancer worldwide. BCC is most prevalent in elderly men. However, susceptibility for men and women increases after age 40, though younger adults are occasionally affected. In addition, those with lighter skin complexion are more susceptible to the development of BCC.
SIGNS AND SYMPTOMS
There are several types of BCC, which vary in their appearance and clinical course. Nodular BCC is the most common form. Nodular BCC appears as a pearly, nearly transparent, dome – shaped papule with visible telangiectasia (dilated capillaries and small blood vessels), which people often mistake for a pimple. The lesion slowly grows over time, can flatten in the middle or stay convex and develop a lifted, pearly peripheral edge. It often ulcerates, bleeds or gets covered with a scab. Superficial basal cell carcinoma is the least aggressive form of BCC. Superficial BCC occurs more commonly on the trunk and extremities. It takes the form of a slightly scaly, irregular, well – demarcated reddish plaque that can imitate psoriasis, eczema, Bowen or Paget disease. Morpheaform BCC is the least frequent type of the condition. In its course, smooth, pale, whitish or yellowish papules occur, hence they can be hard to spot by the patient. Sometimes, basal cell carcinoma can be pigmented and therefore strongly resemble a melanoma.
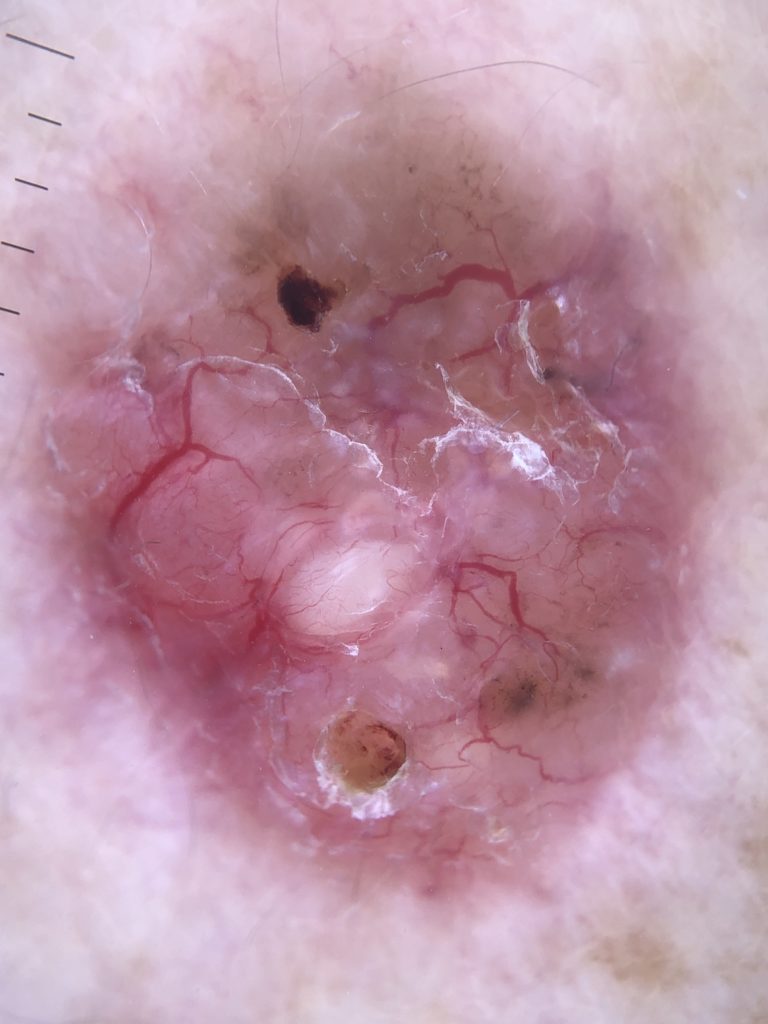
DERMOSCOPY
BCC can contain lots of melanin, becoming pigmented, making it difficult for a diagnostician to differentiate it from other pigmented lesions clinically. Dermoscopy greatly improves the provider’s ability to detect even the smallest BCCs. This non – invasive technique enables the
medical professional to distinguish pigmented BCC from other conditions as well. The dermoscopic features of pigmented basal cell carcinoma include:
• absence of pigmented network
• specks of brown and grey pigment
• numerous blue – grey globules
• linear and branching telangiectasia
• structureless, peripheral leaf – like areas
• focal ulceration.

TREATMENT OPTIONS
Untreated basal cell carcinoma becomes enlarged, easily ulcerates, and destroys the
surrounding tissues. The chosen treatment option largely depends on its size, location, clinical
type as well as patient’s preferences (cosmetic outcome, risks, and wound care). Nodular,
infiltrative and morphoeic BCCs are usually subject to a surgical excision where besides the
cancerous tissue, a 3 – 5 mm margin of healthy tissue is also removed to prevent any relapses in
the future. Mohs microsurgery remains a very effective option, especially when BCC affects
high – risk areas like skin around the eyes, lips and nose. Small, well – defined nodular and
superficial BCCs can be treated using the techniques of superficial skin surgery including highly
successful electrosurgery. If the surgical treatment is inappropriate in one’s particular case,
other options can be incorporated like radiotherapy, photodynamic therapy or topical immune
response modifiers like imiquimod (Aldara®) or 5 -fluorouracil (Efudex®, Tolak®). Pennsylvania
Dermatology Specialists will closely examine your case and assess the most beneficial individual
treatment option.