
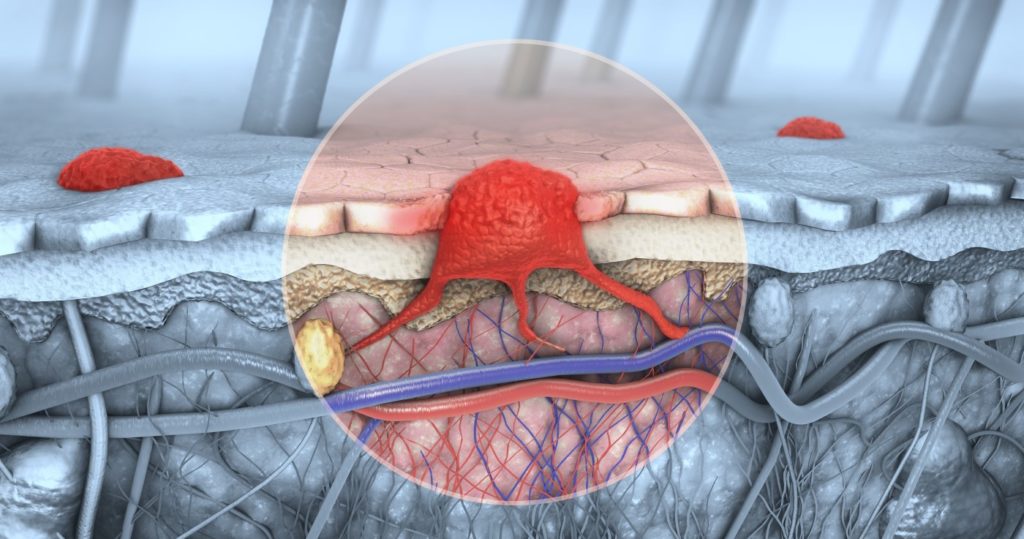
Malignant Melanoma
Melanoma is a form of skin cancer derived from melanocytes – skin cells that produce the skin pigment called melanin. Terms “melanoma” and “malignant melanoma” are used interchangeably. Melanoma is the most aggressive form of skin cancer, and can metastasize to other organs.
EPIDEMIOLOGY
Every year, the number of confirmed melanoma cases around the world rises. It mostly occurs in adults, and very rarely can appear in children. The predisposing factors include: increasing age, history of sunburns, previous malignant melanoma or another type of skin cancer, atypical nevi syndrome, positive family history, multiple melanocytic nevi, lighter skin tones, and immunosuppression. While most melanomas arise de novo, 30% of cases develop from preexisting skin lesions, like lentigines (plural of lentigo or “sun spot”) or atypical nevi, so it is not necessarily reassuring if a lesion in question has been present for years.
WHAT CAUSES MALIGNANT MELANOMA?
Malignant melanoma forms when an uncontrolled, uninhibited proliferation of melanocytic stem cells that had undergone a genetic transformation, takes place. This can be triggered by ultraviolet radiation and other contributing factors. SIGNS AND SYMPTOMS There are several subtypes of malignant melanoma. Superficially spreading melanoma is the most common form, found mostly on the skin of the trunk and the extremities. The lesions are usually flat, asymmetric, and irregularly pigmented. They tend to spread peripherally. Nodular melanoma constitutes approximately 10 – 15% of melanoma cases. Nodular melanoma appears as a fast – growing, brownish or black papule, most frequently found on the extremities. Lentigo – derived melanoma (lentigo maligna melanoma) tends to develop for years on sun-exposed skin, most commonly on the face. Lentigo maligna melanomas appear as flat, brownish, irregularly pigmented, and spotted macules. Acral lentiginous melanoma, is a form of melanoma occurring on the palms of the hands, soles or the feel, or on the nails. This form of melanoma is more common in those with darker skin tones. Melanomas on the nail present as linear, brownish or black pigmented lesions that can be seen through the nail plate.



Malignant melanoma is diagnosed based on the results of a skin biopsy, extracted with a margin of healthy tissue. Two most important prognostic measures are the thickness of the lesion, and presence of ulceration. The former is assessed using the Breslow scale – it measures the thickness of the tumor from its most superficial layer to the deepest point of involvement. The thicker the melanoma, the more likely it is to metastasize. For this reason, during a dermatological consultation, local lymph nodes also should be examined. Those which are easily palpable, should be subject to a biopsy as well. Confirmed malignant melanoma should be surgically excised with a margin of healthy tissue, which depends on the form of melanoma and Breslow thickness. In more widespread, extensive cases other options are available, including Interferon – 2 therapy or various forms of genetic therapy like incorporating BRAF and/or MEK inhibitors. Long – term, regular follow – up observation of the progression of the disease is necessary. Pennsylvania Dermatology Specialists will thoroughly analyze your particular case and come up with the most effective option possible.