Melasma
WHAT IS MELASMA?
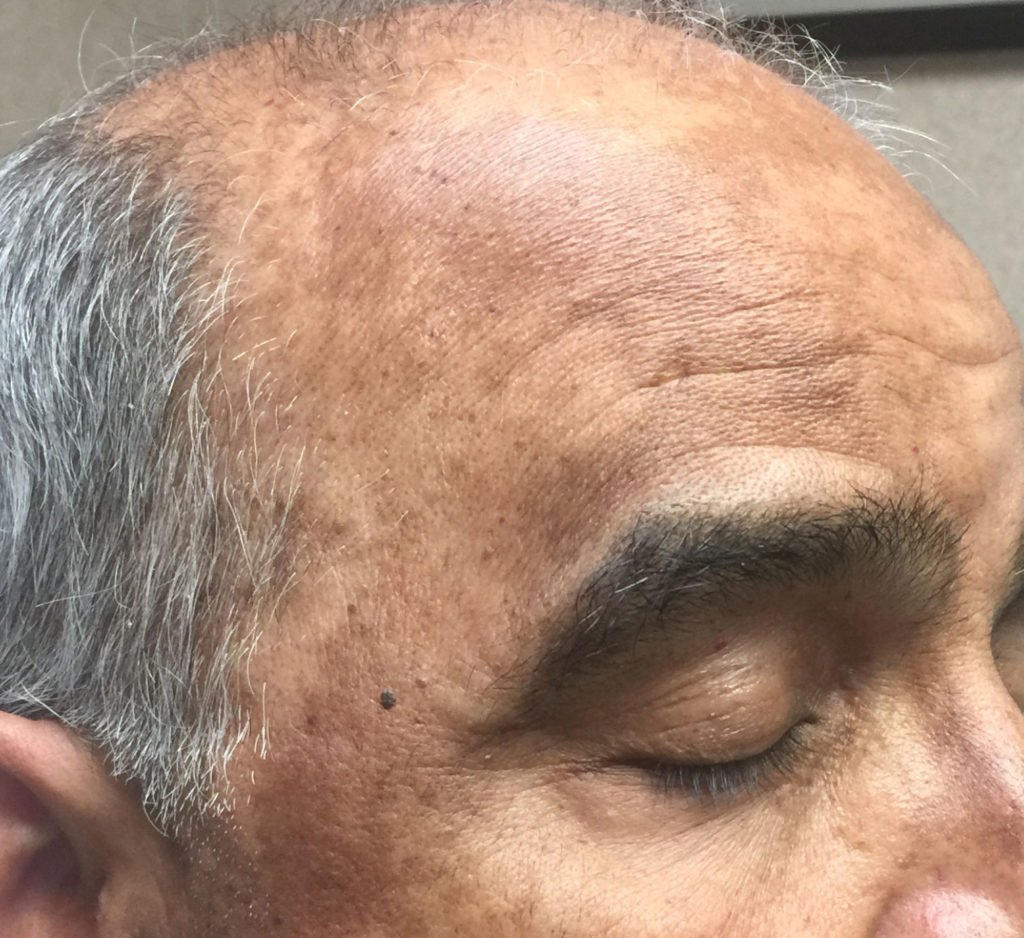
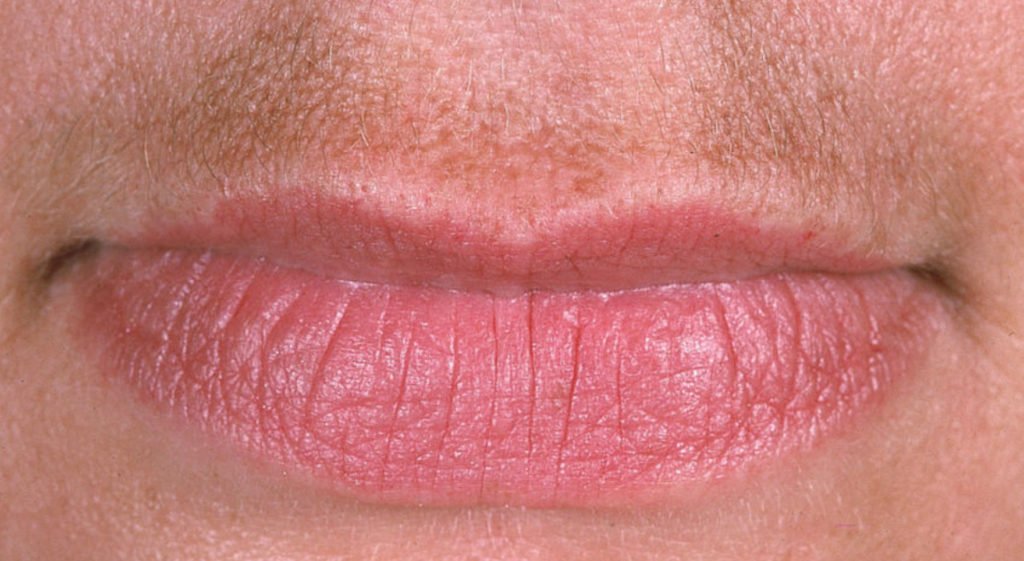
Melasma is either a transient or chronic condition, resulting in hyperpigmentation of the skin. Most often, it affects the skin of the face including the forehead, cheeks, around the eyes, or above the upper lip.EPIDEMIOLOGY
The disorder occurs more frequently in women than in men. The age of onset is typically between the ages of 20 and 40 years old, but can occur in childhood or in middle age. Pregnancy is a common trigger for the condition, due to hormonal changes. However, it is not uncommon for melasma to arise in healthy, non-pregnant adults as well. Other predisposing factors include: darker skin tones (Fitzpatrick skin types 3 and 4), sun exposure and damage, positive family history, as well as hormone medicaments (oral contraceptives), or hypothyroidism.WHAT CAUSES MELASMA?
Melasma is the result of increased activity of melanocytes, which are the cells responsible for the production of melanin. Melanin is the pigment you see in the skin. Subsequently, excess melanin accumulates in the skin, causing local hyperpigmentation. While the exact trigger of increased melanocyte activity is unknown, it has been postulated that an increase of melanocyte-stimulating hormone (MSH) levels, accompanied by higher levels of estrogens and progesterone play an important role.SIGNS AND SYMPTOMS
Melasma often is a singular, well – demarcated, brown macule but sometimes consists of multiple, symmetrical spots on the skin. A macule is a lesion at the level of the skin – it cannot be felt when you touch it, like a freckle.GENERAL DAILY MEASURES
- Wear a year – round high SPF (50+) sun protection, and reapply every 80 minutes. For better results, use a broad – brimmed hat, and seek shade when possible.
- Use a gentle, dermatologically tested cleanser as well as a non – comedogenic moisturizer.
- Consult it with your doctor if hormone therapy should be appropriately adjusted or stopped.