Squamous Cell Carcinoma
WHAT IS SQUAMOUS CELL CARCINOMA?
Squamous cell carcinoma is a common, keratinocyte – derived type of invasive skin cancer. It affects either the skin or the mucosa, most commonly affecting the head, neck or the dorsal (top) surface of the hands. It can derive from a precancerous lesion or form de novo without any previous visible predisposition.
EPIDEMIOLOGY
Squamous cell carcinoma is the second most common kind of skin cancer, constituting approximately 20% of all primary skin cancer cases. SCCs are most often found on elderly men, though it can occur in younger adults and females. Those with lighter skin tones are more at risk for SCC. In 90% of males and 80% of females, SCC was located on the head, neck, and the hands. SCCs found on the legs more often occur in women. A correlation between SCC and certain triggering factors has been observed, including smoking, sun damage, previous SCC or another skin cancer, previous cutaneous injury, positive family history, exposure to arsenic, chronic inflammatory condition, immunosuppression and infection with HPV or human papilloma virus.
WHAT CAUSES SQUAMOUS CELL CARCINOMA?
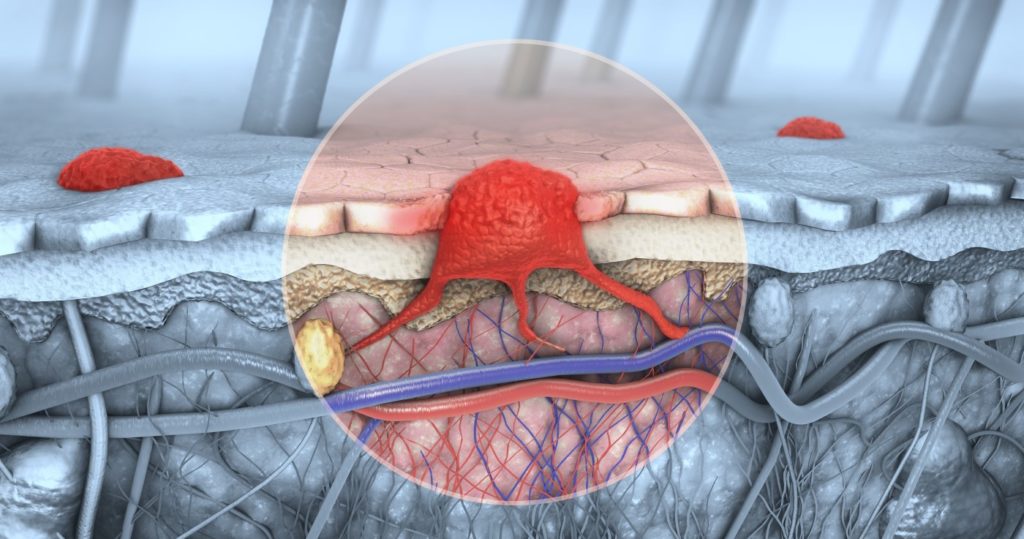
Squamous cell carcinoma forms when an uninhibited, uncontrollable growth of keratinocytes, major skin building cells, takes place. This loss of control of skin cell proliferation is mostly associated with mutations in the tumor suppressor genes. Suppressor genes care for a healthy skin cell proliferation cycle. When these genes mutate, by exposure to ultraviolet radiation or another predisposing factor, they no longer can control the divisions and cancerous growth occurs.


SIGNS AND SYMPTOMS
The disorder typically appears on the skin of body parts most commonly exposed to the sun, especially if the skin has already been damaged by sun rays or is chronically inflamed. Early squamous cell carcinoma can look like a hyperkeratotic, thickened, dome – shaped lesion that resembles actinic keratosis. The lesion then reddens, with an ill-defined base. Untreated primary lesions become enlarged and convex, transforming themselves to hardened, red nodules with a necrotic scab in the center. Eliminating the scab visualizes a cavity filled with deposits of keratin. The lesions can ulcerate and are often tender or painful. Later in the progression, SCC can form metastases to the local lymph nodes, which become enlarged and hardened.